Unmasking Vascular Mysteries: An Opinion on the Challenges in Diagnosing and Treating IVC Lesions
The field of vascular medicine is no stranger to tricky parts, tangled issues, and nerve-racking surprises. As an editor with a deep understanding of modern and complementary medicine, I have found that each case—no matter how routine it may appear at first glance—can unearth subtle parts that force clinicians to figure a path through unexpected turns. Today’s commentary centers on a recent case involving a 57-year-old female whose mechanical thrombectomy was complicated by the extraction of an unsuspected vascular mass, ultimately diagnosed as an inferior vena cava (IVC) arteriovenous hemangioma (AVH). This case serves as a stark reminder of how clinical assumptions can be challenged by confusing bits and fine details that demand careful scrutiny, interdisciplinary collaboration, and a comprehensive diagnostic approach.
Rethinking the Diagnosis: When Thrombus Assumptions Don’t Add Up
At first glance, the patient’s presentation—chest tightness, hypertensive emergency, and elevated cardiac markers—painted a picture consistent with a non-ST elevation myocardial infarction (NSTEMI). However, the incidental detection of an IVC lesion in imaging studies introduced twists and turns that would soon blur the line between a common thrombotic event and a rare vascular anomaly. With various imaging techniques, including transthoracic echocardiography (TTE), computed tomography (CT), and ultrasound, the initial belief was that of a thrombus. But as therapy advanced, the failure of thrombolysis and mechanical clot retrieval pointed to hidden complexities that required a closer look.
This unfolding narrative underscores an important lesson: even when first impressions appear convincing, the underlying pathology may be full of problems that are loaded with issues. Such clinical scenarios are a reminder of the importance of considering the fine shades of diagnostic imaging, clinical presentation, and patient history. When standard protocols come up short, a deeper dive into the subtle parts of the case is essential for patient safety and effective management.
Imaging Insights: Digging Into the Confusing Bits of Vascular Lesion Diagnosis
Modern imaging modalities are super important tools in the identification of vascular anomalies. In the case at hand, initial TTE and CT imaging revealed a suspicious filling defect in the IVC that extended into the right atrium. An abdominal ultrasound further confirmed a non-occlusive echogenic structure, closely resembling a thrombus. However, it was the persistence of the lesion despite aggressive thrombolytic therapy with alteplase and mechanical thrombectomy attempts that made the clinicians step back and dig into the little details.
Comparing Thrombus with Atypical Vascular Masses
When trying to differentiate a common IVC thrombus from an AVH, multi-modal imaging plays a critical role. Consider the following table that highlights some of the key distinguishing features:
| Feature | IVC Thrombus | Arteriovenous Hemangioma (AVH) |
|---|---|---|
| Appearance on Ultrasound | Echogenic structure, often mobile, may occlude blood flow partially or completely | Well-circumscribed mass, with potential vascular channels and flow signals |
| Response to Thrombolytics | Typically shows reduction in size and change in consistency | Generally does not respond due to inherent vascular architecture |
| Histopathology | Fibrin deposits, inflammatory cells | Arteriovenous shunting, benign vascular proliferation |
| Common Location | Often associated with venous stasis in deep veins | Rare in visceral locations, typically found in soft tissues of head, neck, or extremities |
This table is a reminder that while thrombi tend to exhibit a predictable response to standard treatment, an AVH can easily masquerade as a clot, leading to an ambiguous clinical picture that requires extra efforts to figure a path through.
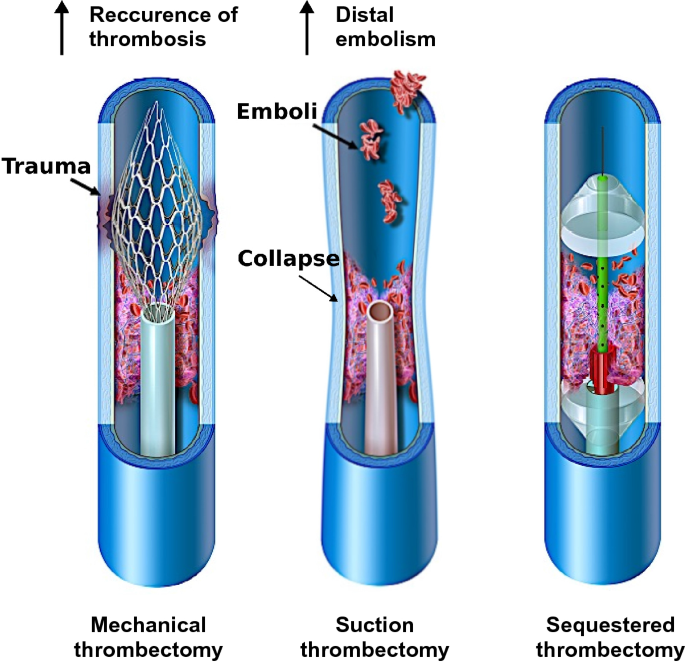
Mechanical Thrombectomy: When Routine Procedures Meet Tangled Issues
The mechanical thrombectomy in this case was intended to clear a suspected clot burden using the Inari FlowTriever and later the Inari ClotTrieverXL system. While these devices serve as key instruments in the modern treatment of venous thromboembolisms, the unexpected retrieval of an elongated, lobular mass instead of the envisioned clot highlights the nerve-racking unpredictability that sometimes accompanies even the most standardized procedures.
Procedure Challenges and Unexpected Findings
During the intervention, the catheter became trapped at the right groin access site—a complication that is not unfamiliar but is nevertheless intimidating. The team’s effort to free the catheter led to the unexpected extraction of a vascular mass that, upon further investigation, was shown to be an AVH. Such moments underscore the importance of staying alert to the possibility that the presumed diagnosis may conceal a broader spectrum of pathology.
Key bullet points regarding the procedural challenges include:
- Initial failure of mechanical retrieval with standard devices.
- Necessity to switch treatment methods amid an ambiguous lesion response.
- Encountering a catheter entrapment that highlighted the twisted parts of the intervention.
- Subsequent need for histopathological analysis to clarify the nature of the retrieved mass.
The eventual deformation of the ClotTriever device served as a tangible reminder of the minimal tolerance for error in such procedures. The mechanical stress experienced underscores the need for rethinking our approach to IVC lesion management when standard clues come up short.
Alternative Perspectives: Reassessing the Use of Thrombolytics in Complex Cases
Part of the debate within contemporary vascular interventions is how to steer through cases where common treatments might worsen the situation. In this scenario, the use of alteplase—to dissolve the presumed clot—proved ineffective. Given the patient’s history of intracranial hemorrhage, this approach was particularly nerve-racking to implement. However, clinicians must sometimes take that chance to manage what appears to be a life-threatening condition, even as they remain aware of potential side effects.
Considerations for Thrombolytic Therapy
Before starting thrombolytic treatment, clinicians must carefully weigh the benefits and risks. Some key factors in such a decision include:
- Patient history (such as prior hemorrhagic events).
- Extent and location of the lesion.
- Potential for misdiagnosis when faced with unusual imaging findings.
- Availability of alternative mechanical strategies.
In this case, the decision to proceed was based on evidence pointing toward a thrombus, yet the final results led the team to revisit their initial assumptions. Such experiences highlight the need to always keep alternative diagnoses on the table, a notion that is both practical and, at times, counterintuitive in our fast-paced medical environment.
Reflections on the AVH Diagnosis: A Rare Encounter in the IVC
The final definitive diagnosis—a benign arteriovenous hemangioma—was based on histopathological analysis that involved immunohistochemical staining using markers such as desmin, CD34, pan cytokeratin, PAX8, and HMB45. Given that AVHs predominantly reside outside the central venous system, their identification in the IVC is extremely rare. This finding should prompt us to dig into the fine points of case categories where vascular malformations are not immediately suspected.
Key Features of AVH in the IVC
The rarity of an AVH in such a central location provides several thought-provoking discussion points for both clinicians and researchers. First, while AVHs normally occur in soft tissue regions like the head and limbs, finding one in the IVC forces us to consider it in the differential diagnosis when faced with atypical presentations. Moreover, this case underscores the following:
- The necessity to keep a wide differential diagnosis for intravascular filling defects.
- The importance of multimodal imaging to reduce the risk of misdiagnosis.
- Understanding that not every vascular mass is a thrombus or neoplasm, but sometimes a benign anomaly.
This emphasis on detailed histopathological evaluation and cross-specialty collaboration is key in arriving at a correct diagnosis in cases loaded with issues. It further elucidates the small distinctions that separate a common clot from an unusual benign vascular mass—distinctions that demand both caution and creative problem-solving on the part of the healthcare team.
The Role of Multidisciplinary Collaboration: Getting Into the Nitty-Gritty of Patient Care
One of the most important lessons from this case is the importance of multidisciplinary collaboration. When faced with confusing bits and tangled issues that resist resolution via one mode of treatment, it becomes super important to bring together experts from various fields, including interventional radiology, cardiology, vascular surgery, and pathology. Each specialist contributes subtle insights that, when combined, help to paint a complete picture of what exactly is happening inside the patient’s body.
Team Approach: Who Should Be Involved?
The following bullet list summarizes the key players and their roles in challenging vascular interventions:
- Interventional Radiologists: Responsible for the imaging-guided procedures and mechanical interventions.
- Cardiologists: Manage overall cardiac function and decide on the immediate treatment protocols for myocardial events.
- Vascular Surgeons: Provide insights into the possible surgical interventions should minimally invasive methods fail.
- Pathologists: Crucial for diagnosing unusual lesions through microscopic assessment and immunohistochemical markers.
- Critical Care Specialists: Monitor and manage the patient’s condition during high-risk post-procedural periods, especially when thrombolytic therapy is involved.
This team-based approach not only helps in pinpointing the cause of a filling defect in high-stakes, nerve-wracking circumstances but also facilitates a more holistic treatment plan. In a way, it mirrors the collaborative spirit that is necessary in all fields of medicine today, ensuring that the patient receives care that is as calculated as it is compassionate.
Taking the Wheel: Lessons Learned from a Case of Vascular Mass Extraction
The case of the IVC AVH challenges long-held assumptions on several levels. Most notably, it drives home the point that not every filling defect in the IVC can be attributed to a blood clot. Instead, it brings to light the need to consider alternative vascular anomalies when faced with obstructions that do not respond to conventional therapies. This is a wake-up call for healthcare providers to continuously question and re-assess their initial diagnostic impressions.
For clinicians, these discussions are not just academic. They have real-life implications on how procedures are planned and executed in the angiography suite and beyond. Below are some of the key take-home messages from this case:
- Always keep an open mind when imaging studies reveal ambiguous lesions.
- Consider alternative diagnoses such as vascular malformations alongside thrombotic processes.
- Review patient history comprehensively before deciding on thrombolytic therapy, especially in patients with prior hemorrhagic events.
- Employ a range of imaging modalities to get around misleading or incomplete data from any single source.
- Ensure that multidisciplinary teams are involved early on in the diagnostic process to provide diverse perspectives on management strategies.
The ultimate goal must always be to reduce the risk of further complications by identifying what lies beneath the surface of typical clinical presentations. This case is a potent reminder that even in a single patient encounter, there can be numerous small twists that, if recognized and managed appropriately, can lead to vastly improved outcomes.
Revisiting Imaging Techniques: Small Distinctions That Matter
One of the most important facets of modern vascular medicine is the use of multiple imaging techniques to identify and characterize lesions. Each modality, be it ultrasound, CT, or TTE, contributes a unique view, aiding clinicians in piecing together a comprehensive diagnosis. However, each method also has its limitations, which, if not carefully balanced, can lead to misinterpretations that complicate the treatment plan.
Imaging Modalities: A Closer Look
Here is a brief overview of the imaging modalities that played a role in the discussed case, along with their benefits and limitations:
| Modality | Benefit | Limitation |
|---|---|---|
| Transthoracic Echocardiography (TTE) | Non-invasive evaluation of cardiac structures and rapid detection of intracardiac masses | Limited in tissue characterization and spatial resolution for extracardiac lesions |
| Computed Tomography (CT) | High-resolution imaging with contrast enhancement provides detailed views of vascular structures | Sometimes inconclusive when differentiating between thrombus and vascular tumors |
| Ultrasound | Real-time imaging capability, widely available, and cost-effective | Operator dependent and can be limited by patient body habitus or suboptimal acoustic windows |
| Venography | Direct visualization of venous structures and flow dynamics | Invasive nature and risk of complications if not performed meticulously |
Each of these techniques contributed a piece to the overall puzzle. When working through a case filled with challenging aspects, combining these diagnostic tools is not only pragmatic but downright necessary. The combined expertise of radiologists and clinicians ensures that subtle parts—those that might otherwise be overlooked—are brought to light, paving the way for more informed treatment decisions.
Finding Your Path Through Uncertain Diagnoses: The Importance of Staying Adaptable
One of the lingering lessons of this case is that medicine is often a process of sorting out twist after twist. Even when the clinical picture seems straightforward, hidden complexities can emerge. The transition from the initial diagnosis of a regular IVC thrombus to the eventual recognition of an AVH underscores the importance of maintaining an adaptable approach to treatment.
Adaptability in Clinical Decision-Making
Clinical protocols are designed for standard presentations, yet every patient is unique. When standard treatments yield confusing results or when procedures like mechanical thrombectomy encounter tangled issues, the following strategies can help clinicians get into the nitty-gritty:
- Re-assess the initial diagnosis using a combination of repeat imaging and new data from interventions.
- Engage specialists from various fields to offer different perspectives on ambiguous findings.
- Consider the full spectrum of differential diagnoses, including less common entities like AVH.
- Remain prepared to switch therapeutic strategies quickly when existing methods do not yield expected outcomes.
This agile mindset is particularly critical in vascular medicine where decisions must be made rapidly and accurately. The case clearly shows that when clinicians find themselves faced with nerve-racking scenarios, the key lies in being ready to re-adjust the treatment plan and to appreciate those small distinctions that may ultimately change patient management.
Implications for Future Practice: Embracing a Comprehensive Diagnostic Approach
As the medical community continues to advance, cases like the one discussed offer critical insights that should be integrated into future practice. The experience not only calls into question the reliance on conventional assumptions but also emphasizes the need for thorough diagnostic procedures that consider even the most unlikely possibilities.
Integrating Lessons Learned into Clinical Workflows
To make sure that we are well-prepared for similar cases in the future, several key steps should become standard practice:
- Enhanced Imaging Protocols: Utilize a combination of imaging techniques early in the diagnostic process, particularly when the initial findings hint at possible alternative diagnoses.
- Robust Multidisciplinary Meetings: Foster close collaboration among radiologists, cardiologists, vascular surgeons, and pathologists to review challenging cases and to share insights from different perspectives.
- Dynamic Treatment Strategies: Remain open to changing the course of treatment when the expected therapeutic response does not occur, ensuring that unusual findings are addressed immediately.
- Continued Education and Training: Regularly update clinical teams with recent findings in vascular anomalies and alternative pathologies, promoting an environment where suspicious cases are thoroughly re-evaluated.
- Patient-Centered Decision Making: Particularly in high-risk cases like those involving previous hemorrhagic events, ensure that every decision is weighed with the patient’s safety in mind.
Embracing this comprehensive approach not only improves diagnostic accuracy but also serves as a safeguard against unexpected risks. By factoring in both the obvious and the hidden complexities, clinical practitioners can better manage the delicate interplay between established protocols and the need to adapt to individual patient challenges.
Reflections on Patient Safety: Balancing Risk and Innovation
The case of the IVC AVH is more than just a medical oddity—it is a complex narrative that highlights the importance of balancing risk and innovation. With treatments like thrombolytic therapy carrying their own set of challenges, especially in patients with contraindicating medical histories, the margin for error becomes extremely narrow. Here, the benefit of exploring unconventional diagnoses must be carefully weighed against the potential risk of over-treatment or misdirected therapy.
Strategies to Ensure Patient Safety
In sorting out nerve-racking clinical decisions, the following strategies are essential:
- Rigorous Pre-Procedure Assessment: Evaluate patient history and risk factors thoroughly, especially in those with previous bleeding events or other contraindications.
- Real-Time Monitoring: Implement continuous monitoring during and after procedures, ensuring swift detection of any adverse developments.
- Contingency Planning: Prepare backup strategies for situations where standard interventions fail, including additional imaging and expert consultation sessions.
- Clear Communication: Maintain open channels between all members of the care team to ensure that any unexpected finding is rapidly shared and addressed.
By carefully weighing these considerations, healthcare teams can better manage the challenging pieces of unexpected pathology while minimizing risk. In turn, this fosters an environment where innovation in diagnostic and therapeutic techniques is encouraged—provided it is matched by a robust safety net.
The Future of Vascular Interventions: Learning from the Past to Shape Tomorrow
Every challenging case in the domain of vascular interventions adds a valuable chapter to the evolving story of medicine. The experience of handling an IVC lesion that turned out to be an AVH fundamentally shifts our understanding and encourages us to consider rare vascular anomalies in our routine differential diagnoses. With modern imaging and evolving procedural technologies, there is immense potential not only to improve treatment outcomes but also to refine our diagnostic algorithms.
Looking Ahead: Opportunities for Improvement
Looking forward, several opportunities emerge for enhancing our approach to cases like these:
- Advanced Imaging Techniques: Research into higher-resolution imaging and real-time diagnostic tools can help differentiate between thrombi and benign vascular anomalies even more effectively.
- Device Innovation: Improvements in thrombectomy devices that can better adapt to and manage unexpected tissue properties could reduce instances of device deformation and catheter entrapment.
- Data-Driven Protocols: Incorporating data analytics and machine learning to analyze large sets of imaging results may soon help predict when a lesion is atypical, guiding clinicians toward alternative treatment paths earlier in the process.
- Enhanced Training Programs: Developing comprehensive training modules that include rare case studies will prepare future clinicians to spot and manage these unusual presentations with confidence.
By learning from the past and staying receptive to innovative approaches, the medical community can continue to make strides in the diagnosis and management of vascular anomalies. This balanced approach—one that celebrates cutting-edge technology while respecting the wisdom gained from challenging cases—will ultimately benefit patients by reducing the risk of misdiagnosis and enhancing treatment outcomes.
Final Thoughts: Embracing the Unexpected on the Road to Improved Care
In conclusion, the case of a mechanically retrieved IVC lesion, later identified as an arteriovenous hemangioma, is a powerful lesson in humility, adaptability, and thorough diagnostic rigor. It underscores the importance of being prepared for the nerve-racking moments when expected treatments confront confusing bits of unexpected pathology. More importantly, it reminds all of us—the clinicians, researchers, and healthcare enthusiasts—that even in an era dominated by advanced imaging and streamlined procedures, the human element of curiosity, collaboration, and caution remains absolutely essential.
This experience compels us not only to take a closer look at ambiguous intravascular filling defects but also to continue engaging in open, multidisciplinary dialogue. By working through each tangled issue—whether through re-assessment of imaging, adoption of alternative interventions, or leveraging the fine details provided by histopathology—we can better ensure that our patients receive a level of care that is both innovative and safe.
Ultimately, as we reflect on this experience, let us remember that medicine is a journey full of twists and turns. The unexpected sometimes becomes the catalyst for progress, pushing us to question established notions, and driving us to find your way through even the most intimidating challenges. By embracing these challenges with thoughtful analysis and collaborative problem-solving, the future of vascular interventions looks not only promising but also prepared to tackle the hidden complexities that lie ahead.
Originally Post From https://www.cureus.com/articles/349356-mechanical-thrombectomy-complicated-by-vascular-mass-extraction-a-case-of-inferior-vena-cava-arteriovenous-hemangioma
Read more about this topic at
Mechanical Thrombectomy Complicated by Vascular Mass …
Persistent Thrombotic Hemangioma With Organizing/ …