Introduction: A New Perspective on Adjunctive MMAE for Chronic Subdural Hematoma
The management of chronic subdural hematoma (cSDH) is full of tricky parts and tangled issues that continue to capture the attention of neurosurgeons and interventional radiologists alike. As treatment options evolve, the use of middle meningeal artery embolization (MMAE) as an adjunct to surgical evacuation has stirred conversation in both academic and clinical circles. In this editorial, we take a closer look at the order and timing of MMAE relative to surgery, discussing the current evidence, practical considerations, and areas where further research is super important. This discussion is designed to help clinicians find their way through the confusing bits and fine points of this evolving treatment paradigm.
While traditional surgical evacuation—whether by craniotomy, burr hole drainage, or even subdural evacuating port system placement—has been the mainstay of treatment for cSDH, recurrence rates can be nerve-racking. MMAE has emerged as a minimally invasive method intended to reduce recurrence by targeting the blood supply to the subdural collection. Yet, questions remain regarding the optimal timing of the embolization step: Should it be performed before surgery to improve efficacy, or after surgery to address any residual issues?
Understanding Chronic Subdural Hematomas and Treatment Pathways
Chronic subdural hematoma represents a slow accumulation of blood between the brain’s covering layers, a condition that predominantly affects older individuals. The clinical presentation may be subtle and sometimes overwhelming in its variability. In many cases, patients present with nonfocal symptoms that can progressively impact quality of life over weeks. The decision whether to manage these lesions operatively or nonoperatively depends on a range of factors such as hematoma thickness, midline shift on imaging, and the patient’s overall functional status.
Even though surgical evacuation has been the traditional treatment, the procedure is sometimes laden with confusing bits and nerve-racking outcomes—especially when recurrence occurs. In this context, the adjunctive role of MMAE has become an area of considerable interest among practitioners who are eager to figure a path through the tangled issues associated with recurrence.
Exploring the Role of Middle Meningeal Artery Embolization
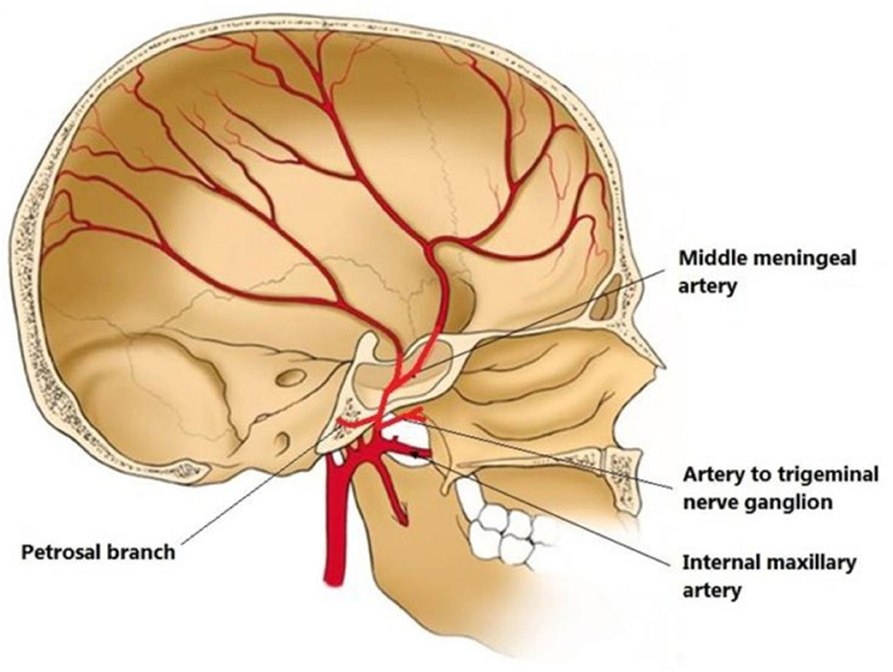
MMAE works by interrupting the blood supply to the membrane responsible for sustaining the hematoma. By embolizing the middle meningeal artery, clinicians aim to promote the resorption of the hematoma and reduce the chance of reaccumulation. This approach is less invasive compared to traditional surgical techniques and may offer advantages in patients who are at increased risk for surgical failure or recurrence after initial evacuation.
For many practitioners, the idea of using a catheter-based intervention to target the artery has its own set of little details and subtle parts. On the one hand, it can make patient management more efficient; on the other, technical and timing considerations have made the approach feel a bit off-putting in some settings. Yet, with improved techniques and better imaging guidance, MMAE is steadily gaining ground as a super important tool in the neurosurgical armamentarium.
Timing of MMAE: Before Surgery or After?
One of the most debated issues in the use of adjunctive MMAE for cSDH is whether it should be performed before surgical evacuation or after. Both strategies have been employed in clinical practice, with the aim of reducing recurrence rates and improving patient outcomes. However, the tricky parts of determining the best timing often require clinicians to balance potential benefits against the nerve-racking risk of suboptimal results.
Recent studies, including multicenter analyses, have compared outcomes between MMAE performed before surgery and those where it is performed afterwards. Although the available data have not shown any statistically significant differences in reoperation rates or technical success based solely on the order of MMAE relative to surgery, many clinicians remain cautious.
Weighing the Options: Preoperative Versus Postoperative Embolization
Performing MMAE before surgery is often favored by teams that want to ensure the distal branches of the middle meningeal artery are open for optimal embolization. In contrast, those who deal with patients needing emergency surgical intervention due to large hematomas or significant midline shift may opt to perform MMAE afterwards to address any persistent bleeding risks.
Key points to consider include:
- Preoperative MMAE: May allow for better penetration of embolic agents into the target vessels; however, it requires careful planning and coordination.
- Postoperative MMAE: Offers the flexibility to manage patients with emergent presentation, yet may be complicated by changes in vascular anatomy following surgery.
Both strategies aim to reduce the need for reoperation and minimize recurrence, and the evidence so far suggests that either approach can be effective when tailored to individual patient needs.
Early Versus Late MMAE: A Closer Examination
Beyond the simple dichotomy of before versus after surgery, another layer of complexity emerges when considering the interval between surgery and MMAE. Clinicians may perform the embolization within two days of surgery or opt for a slightly delayed approach, 3–7 days later. Again, studies have shown that outcomes—in terms of reoperation rates and technical success—do not significantly differ between early and late timing groups.
This finding is particularly relevant for those managing their way through surgical scheduling and resource utilization challenges. It alleviates concerns that a nerve-racking delay might compromise the effectiveness of MMAE.
Interpreting Outcome Data for Different Timing Strategies
In recent multicenter studies:
- Reoperation Rates: Ranged between approximately 4% and 7% regardless of the timing, suggesting that both early and late MMAE are viable options.
- Technical Success: Achieved success rates between 97% and 100%, indicating that the procedure itself is reliably performed when conducted by experienced teams.
Such findings underscore that while the choice of timing might appear intimidating at first, its actual impact on key outcomes may be modest. That said, these studies were underpowered to detect small differences; thus, the real-world differences might be more nuanced than the available data suggests.
The Evidence from Recent Multicenter Studies
A collaborative multicenter study across 10 U.S. centers assessed 266 MMAE procedures in more than 230 patients. The study compared outcomes in patients who underwent MMAE before surgery with those who had the procedure afterwards, as well as comparing early versus late postoperative timing. The evidence, though not definitive in showing significant differences, provides valuable insights into the feasibility and safety of both approaches.
Below is a simplified table summarizing some of the key findings from these analyses:
| Outcome | Preoperative MMAE | Postoperative MMAE |
|---|---|---|
| Reoperation Rate | Approximately 5% | Approximately 7% |
| Technical Success | Nearly 100% | Approximately 97% – 98% |
| Procedure Duration | Slightly shorter on average | Slightly longer on average |
| Radiographic Success | High rates noted | Comparable outcomes |
This table illustrates that while there may be slight differences in procedural duration and radiographic outcomes, both approaches show promising success rates and acceptable reoperation figures. Many of the differences do not reach statistical significance, suggesting that MMAE is robust to variations in timing, at least within the range studied.
Technical Success and Reoperation: What Do They Mean in Practice?
Technical success is defined by the ability to achieve the desired embolization without complications. Reoperation rates, on the other hand, reflect the need for additional interventions due to recurrence of the hematoma. In the studies reviewed, a technical success rate nearing or hitting 100% points to a well-mastered procedure with minimal room for error. Similarly, low reoperation rates provide reassurance that adjunctive MMAE is providing a durable benefit.
Despite these optimistic findings, some critics argue that the studies may be underpowered—that is, they might not detect subtle but clinically meaningful differences. While this critique is valid, the overall trend remains reassuring for practitioners who are contemplating the timing of MMAE in their practice.
Considerations for Clinical Practice
The real challenge for clinicians lies in applying these research insights to everyday practice. The decision to perform MMAE before or after surgical evacuation must consider a range of factors, including patient-specific variables, logistical constraints, and the availability of expertise and equipment. In many instances, the subtle details of a patient’s overall health, imaging findings, and even anticipated blood loss can steer the decision-making process.
When planning treatment for cSDH, here are some key considerations:
- Patient Age and Comorbidities: Older patients, who form the bulk of the cSDH population, may have additional health issues that complicate surgery or affect the risk-benefit ratio of MMAE.
- Functional Status: A patient’s baseline modified Rankin scale (mRS) score can help determine the urgency and aggressiveness of intervention.
- Prior Surgical History: For patients with a previous surgical evacuation, the risk of recurrence is higher, and adjunctive MMAE might be particularly attractive.
- Anticoagulation and Antiplatelet Use: Medications that affect blood clotting can influence bleeding risk, making the timing of MMAE even more critical.
Integrating these patient-specific factors into the treatment algorithm is essential to managing your way through the tangled issues inherent in cSDH care.
Operational and Logistical Factors in MMAE Timing
The decision regarding whether to perform MMAE before or after surgery is not purely clinical—it also involves working through logistical constraints and resource management within a treatment facility. For example:
- Schedule Coordination: Preoperative embolization requires close coordination between the surgical and interventional teams. This may be challenging in centers where resources are stretched thin or where urgent cases are frequent.
- Procedure Duration and Hospital Stay: Studies have shown that the length of stay and procedural duration may vary based on the timing of MMAE. While these differences may be small, they can have an impact on overall healthcare costs and patient throughput.
- Team Experience: The fine points of MMAE technique, from catheter selection to embolic material choice, demand a well-trained team. Facilities with more experience may be more comfortable performing preoperative MMAE, while others might prefer the safety net of postoperative application.
These operational challenges are by no means insignificant. However, the evidence suggests that both timing strategies are feasible, offering clinicians multiple avenues to approach a nerve-racking condition with confidence.
Potential Benefits and Limitations of Adjunctive MMAE
One of the most compelling cases for the use of adjunctive MMAE in cSDH is its potential to reduce the rates of recurrence—an outcome that has traditionally been a significant source of uncertainty and intimidating complications. Reduced recurrence means fewer reoperations, less overall morbidity, and a smoother recovery trajectory for patients.
In summary, some of the key benefits of adjunctive MMAE include:
- Lower Recurrence Rates: By disrupting the blood supply to the hematoma membrane, MMAE helps decrease the likelihood of reaccumulation.
- High Technical Success: With success rates nearing 100% in experienced hands, the procedure is both reliable and reproducible.
- Improved Radiographic Outcomes: Imaging improvements post-embolization offer measurable evidence of treatment efficacy.
- Flexibility in Timing: The current evidence suggests that both preoperative and postoperative approaches can work, allowing treatment to be individualized.
Despite these benefits, there are limitations to consider. The studies conducted so far have been retrospective and, in many cases, underpowered to detect small but clinically meaningful differences. Additionally, there are potential risks associated with any endovascular procedure—including periprocedural complications—which require careful patient selection and expert procedural skill to mitigate.
Below is a table outlining the potential pros and cons of adjunctive MMAE:
| Pros | Cons |
|---|---|
|
|
Risks and Complications: Weighing the Trade-Offs
Any procedure that involves navigating through the delicate blood vessels of the brain comes with its own set of intimidating risks. With MMAE, the risks are generally low but can include complications like vessel injury, embolic material misplacement, or inadvertent occlusion of unintended arteries.
Although the rate of periprocedural complications in recent studies has been reported as low—hovering around 3% to 4%—the potential for serious adverse events, however small, cannot be ignored. Clinicians must carefully consider these risks in the context of each patient’s profile and the overall expected benefit. In many cases, the small risk may be entirely acceptable when weighed against the potential to significantly reduce recurrence, especially in patients with a history of prior surgical evacuation.
In practical terms, risk management for MMAE involves ensuring that:
- Patients are properly screened for contraindications to the procedure.
- Technical protocols are strictly followed by well-trained teams.
- Contingency plans are in place should complications arise.
This systematic approach helps the clinical team make their way through the nerve-racking potential complications and focus on achieving the best possible outcome for the patient.
Future Directions and Research Needs
While the current body of evidence provides reassurance about the feasibility of both preoperative and postoperative MMAE, there remains much to be understood. Ongoing studies and future research should aim to address the subtle differences in outcomes that might be clinically significant but have so far been difficult to detect due to sample size limitations.
Further investigation into the following areas is critical:
- Randomized Controlled Trials: To definitively compare the two timing strategies and establish standardized protocols.
- Larger Multicenter Studies: These can help capture small differences in outcomes that may currently be lost in underpowered analyses.
- Patient-Specific Outcome Measures: Investigating the role of comorbidities, age, and prior surgical history in determining the optimal timing and approach.
- Use of Advanced Imaging Techniques: To better understand the fine shades of vascular anatomy and tailor the embolization strategy accordingly.
The ultimate goal in future research is to develop a more precise framework that allows healthcare providers to dig into the nitty-gritty of MMAE timing decisions with confidence. Larger studies and randomized data will be super important in confirming preliminary findings and ruling out small differences that might influence clinical practice.
Broadening the Evidence Base: Incorporating Real-World Data
One promising approach to refining our understanding of MMAE in the treatment of cSDH is the incorporation of real-world data. Registries and multicenter collaborations can provide insights that complement controlled trials. Such data can reflect the messy reality of clinical practice, where resource limitations, patient variability, and unforeseen complications play a role.
In this context, practitioners are encouraged to document their experiences meticulously and contribute to larger databases. This collective effort can help to illuminate the subtle twists and turns of MMAE timing and order that individual studies may not capture.
Conclusion: A Balanced View on MMAE Timing in cSDH Management
In summary, the use of middle meningeal artery embolization as an adjunct to surgical evacuation for chronic subdural hematoma represents a promising advancement in the management of a condition historically riddled with complications. The evidence so far suggests that whether MMAE is performed before or after surgery—and whether it is administered early or with a slight delay—both approaches yield comparable outcomes in terms of technical success and reoperation rates.
Even though the current studies do not reveal statistically significant differences between the various timing strategies, it is important to note that they may be underpowered to detect smaller, yet clinically meaningful differences. Therefore, clinicians should continue to assess each case on its own merits, taking into account not only the clinical and radiographic findings but also the operational and logistical challenges that come with different treatment pathways.
The balance between the potential benefits—such as lower recurrence rates and high technical success—and the nerve-racking risks and complications will continue to be a central theme as we work our way through the fine details of managing cSDH. For now, both preoperative and postoperative MMAE remain acceptable strategies, offering flexibility and allowing treatment to be tailored to each patient’s unique circumstances.
Looking ahead, larger prospective studies and randomized controlled trials will be critical to validate these early observations and identify whether even small differences in timing or technique might lead to improved outcomes over the long term. As the evidence base expands, clinicians will be better equipped to figure a path through the confusing bits of cSDH management, ensuring that every patient receives the most appropriate, safe, and effective treatment available.
Ultimately, the choice of MMAE timing should be seen not as a rigid protocol, but as a flexible tool in the clinician’s armamentarium—one that can be adjusted to match the complex, often overwhelming realities of patient care. With continued research and collaboration among neurosurgeons, interventional radiologists, and other specialists, our understanding of this innovative treatment approach will only deepen, paving the way for even better patient outcomes in the future.
Originally Post From https://pubs.rsna.org/doi/10.1148/radiol.241571
Read more about this topic at
Understanding Success Criterion 2.2.3: No Timing | WAI
Not sure what I’m doing wrong with regards to timing.